Covid-19: Is India reporting fewer cases because of lower testing?


India entered a three-week lockdown to tackle the Covid-19 pandemic in the month of March 2020. The first lockdown was announced on 24 March and remained in effect from 25 March 2020 to 14 April 2020. Ever since, attempts have been made to try and understand how India has fared with the coronavirus pandemic and how the country of more than 1.3 billion people has handled it. Experts have tried exploring and explaining the reasons for the slowdown in new Covid-19 cases in India while those in the media have also been asking questions about the same. In November 2020, questionable testing kits were also blamed for the slowing down number of new cases.
For a deeper dive into the issue, it is important to take a closer look at testing and answer the first question that springs to mind: Are the number of new cases falling because of lower levels of testing in the country? We take a closer look at testing in India over this past year. Our analysis shows that even though daily testing numbers have gone up seven and half times between May 2020 and Feb 2021, the number of new cases is down. We also tried to take a closer look at testing across states and find little correlation between testing and urbanization or between testing and affluence.
According to Our World in Data, India has been the second worst affected country in the world (after USA) when it comes to total number of Covid-19 incidences. As on date the total case count in the country stands just shy of 11 million. Nearly 10.5 million of these cases have recovered and there have been 155,080 deaths.
India reported only 3,565 new cases on 4 Feb 2021 (Ministry of Health and Family Welfare, Government of India). India saw similar numbers being reported in the month of May 2020 (3,525 cases reported on 12 May 2020). The highest number of Covid-19 cases that India recorded in a single day was 97,894 on 16 September 2020.
The daily incidences of Covid-19 cases have broadly been on a declining trend since the peak in September 2020.
Is India reporting fewer new cases because of lower levels of testing?
India reported the highest number of new cases (97,894) of Covid-19 infection on 16 September 2020. This was on a day when 1.13 million Covid-19 tests were conducted across the country. The test positivity rate was 8.61%.
Covid-19 testing in India took off slowly with testing kits being imported in the early months (See Figure 1: Covid-19 New Tests – India).
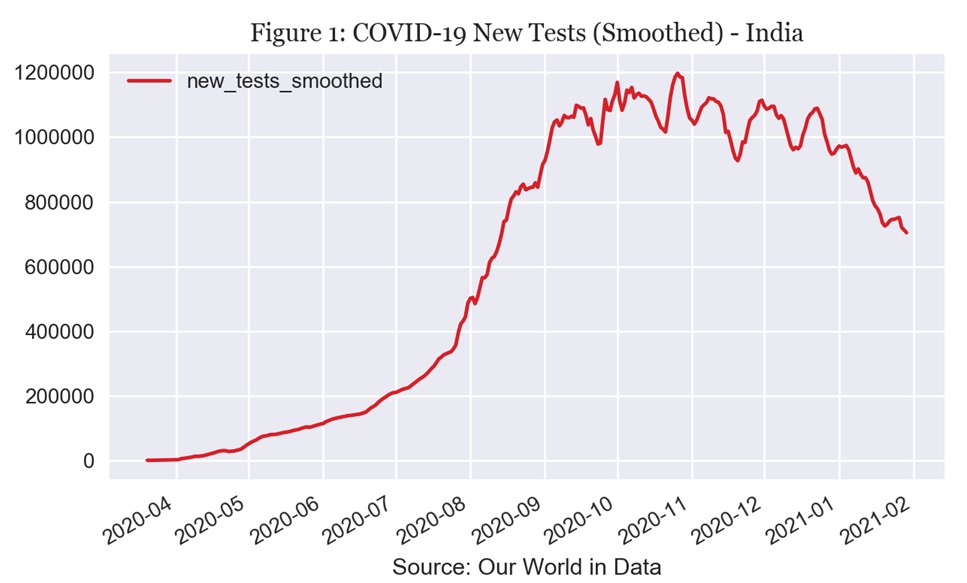
By the end of April 2020, India was conducting 50-60,000 Covid-19 tests per day. 18 May 2020 was the first day when India conducted more than 100,000 tests in a day. Thus, the comparison of daily incidences (new cases) on 4 Feb 2021 (3,565 cases) and 12 May 2020 (3,525 cases) needs to be measured against the number of tests conducted on the day. India conducted 94,671 tests on 12 May 2020 and 715,776 tests on 4 Feb 2021: 7.5 times more.
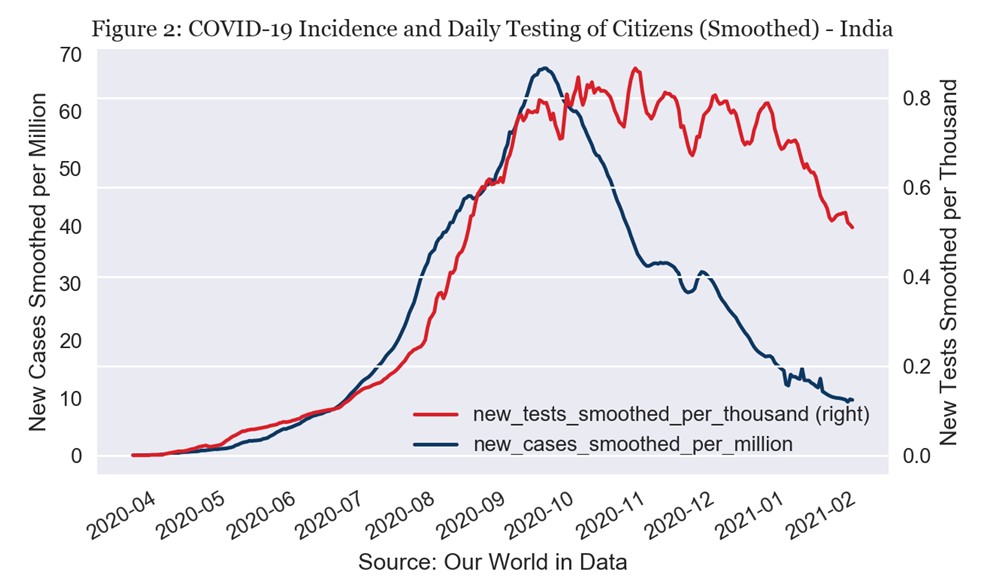
India conducted an average of 94,663 tests per day in the month of May 2020. This increased to 166,313 in June, 339,744 per day in July, 773,102 in August and hit an average of more than 1 million tests per day in September 2020. It peaked at 1.1 million tests per day in October and stayed above 1 million per day in November and December 2020. The number of tests conducted per day decreased to 773,578 per day in January 2021.
The month of September saw India add 2.62 million new cases with a daily average of 87,381. The number of new cases started declining in the month of October (Total new cases: 1.87 million, Daily average: 60,371). This happened despite India testing more in October than any other month so far.
This is clearly demonstrated in the Covid-19 Incidence and Testing chart (Figure 2). The chart shows that while the number of Covid-19 tests conducted in India stayed high between September 2020 and December 2021, the number of new cases added per day started declining in October 2020 itself.
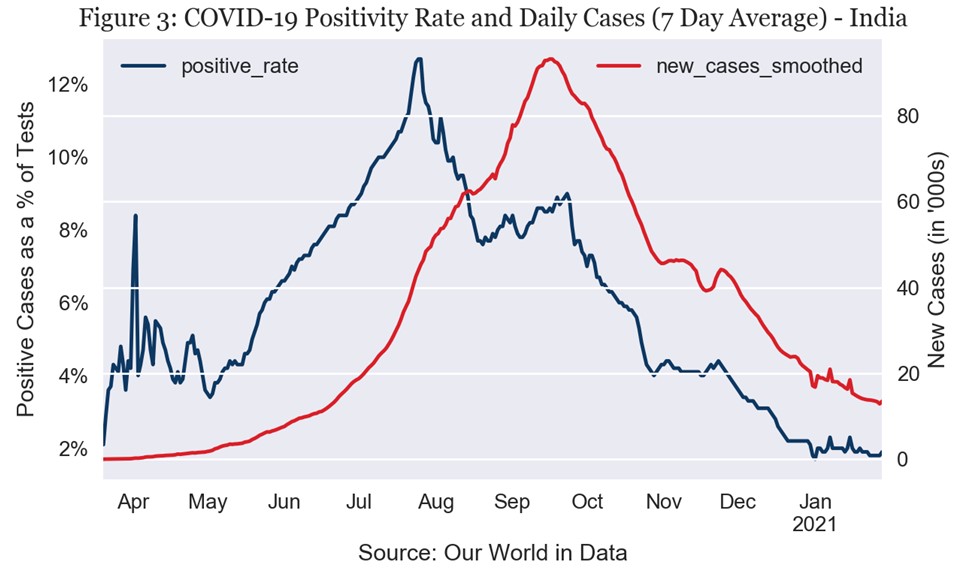
The test positivity rate also points to a weakening pandemic in India. After a peak average positivity rate of 10.6% in July 2020, it came down to 8.62% in August and 8.35% in September. India saw a positivity rate of only 1.98% in January 2021.
Positive percent or positivity rate
In this article, epidemiologists David Dowdy and Gypsyamber D’Souza, explain the importance of the positive percent (or test positivity rate). According to them, “A higher percent positive suggests higher transmission and that there are likely more people with coronavirus in the community who haven’t been tested yet.”
The positivity rate informs us how widespread transmission is in area where testing takes place. Higher positivity points towards the need to test more as transmission may be higher and it aids policymakers in deciding about restrictions.
According to the writers, a positive percent of 5% is considered too high and it must stay below 5% for two weeks before the governments can consider relaxing restrictions.
India has had a positive percentage (positivity rate) of less than 5% since 14 November 2020 (Figure 3). This points to lower levels of transmission since November at a time when India was conducting a million tests every day.
The broad decline in India’s positivity rate since September and the low rate now explain the fewer new incidences of Covid-19 cases being added now.
The decline in new cases can thus be attributed to lower levels of transmission and not to lower levels of testing.
Are states with higher per capita NSDP testing more
Did the states with higher Per Capita Net State Domestic Product (current prices) test more compared to states with lower Per Capita NSDP?
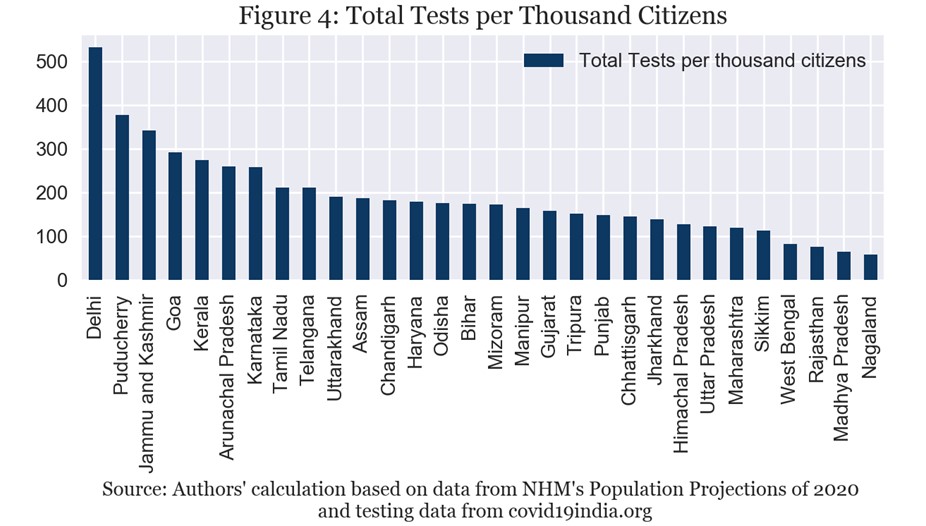
Delhi, Puducherry, Jammu and Kashmir, Goa and Kerala are the top five states in India in terms of the number of tests per thousand of population (Figure 4). Delhi conducted 530 tests per thousand of population while Kerala (at number 5) conducted 270 tests per thousand of population.
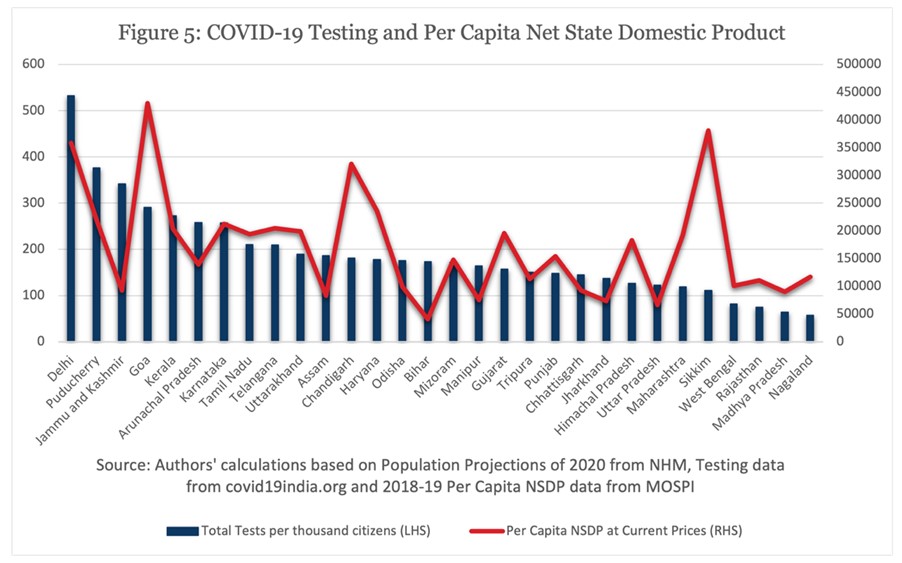
When we plot the total tests per thousand population with the per capita NSDP of the state, we find that no such trend emerges (Figure 5). Take the examples of the Union Territory of Chandigarh and the state of Haryana. On the basis of per capita NSDP, Chandigarh and Haryana are ranked 4 and 5, respectively but on the basis of tests per thousand they are ranked 12 and 13. On the other hand, Jammu and Kashmir is ranked 24 on per capita NSDP basis but is ranked 3 on the basis of tests per thousand.
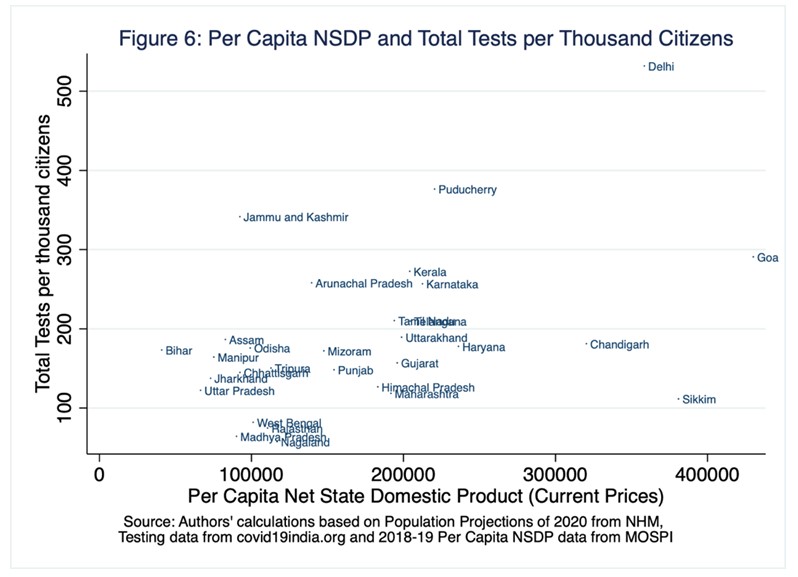
This is observed even more clearly on the scatter plot below (Figure 6). We find that higher per capita NSDP does not necessarily mean higher levels of Covid-19 testing.
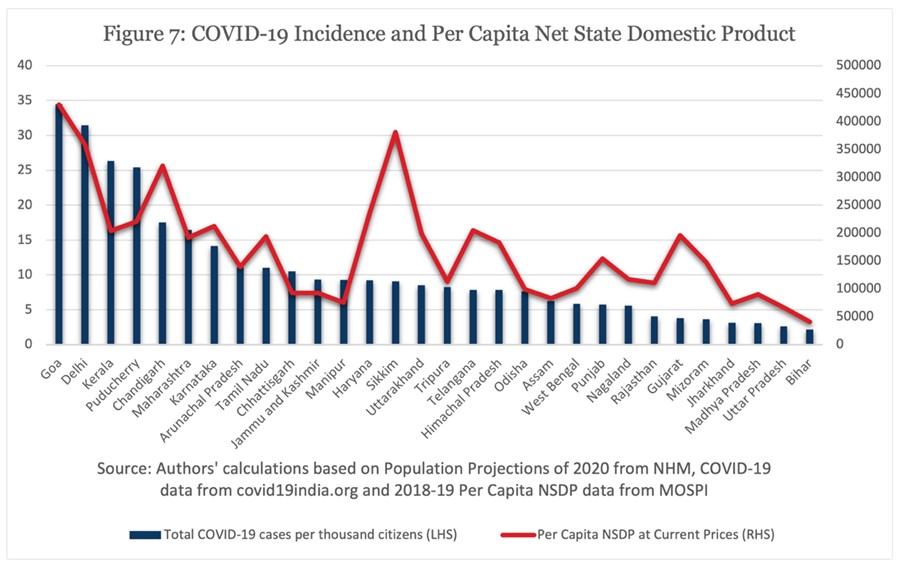
A similar situation is seen when we plot Covid-19 incidence (total cases per thousand) with per capita NSDP in a graph (Figure 7). No discernible trend is seen that can show a strong link between higher Covid-19 caseloads and high (or low) per capita NSDP in the states.
Is there no correlation between state per capita income and Covid-19 though? Pulapre Balakrishnan and Sreenath K. Namboodhiry explored Interstate Variation in Mortality From Covid-19 in India[i] and found that richer states in India had higher case fatality rate (CFR). Case fatality rate is calculated by dividing number of deaths due to Covid-19 by the number of cases detected by testing. In their article, the authors conclude that being wealthy offered no defence against coronavirus in India.
According to the authors, a state’s public expenditure as percentage of state GDP is inversely proportional to per capita income. This explains the higher Covid-19 mortality in richer states as “avoidance of fatality was found to be more closely related to public health expenditure than to infrastructure.”
Is there an urbanization bias to testing in states?
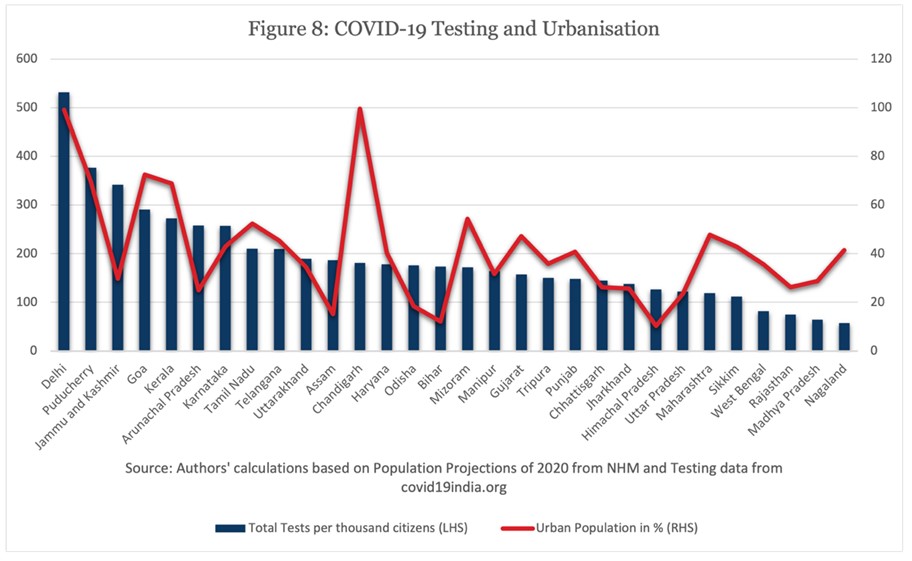
Are states with higher levels of urbanization testing more than those with lower levels of urbanization? We take the tests per thousand population data for states and plot it alongside data for percentage of urban population in states. Delhi and Puducherry find themselves amongst the top ranked states on both parameters. Delhi ranks 1 and 2 on testing and urbanization respectively while Puducherry is ranked 2 and 4. Jammu and Kashmir is the outlier amongst states testing more once again. The state is ranked 20 when it comes to urbanization and ranks 3 when it comes to tests per thousand. Chandigarh, Gujarat and Maharashtra also prove a weak link between urbanization and testing. Chandigarh ranks 1 on urbanization but is ranked 12 on testing. Gujarat ranks 9 on urbanization but 18 on testing. Similarly, Maharashtra ranks 8 on urbanization but 25 on testing.
Thus, we find a weak link between urbanization and testing across states.
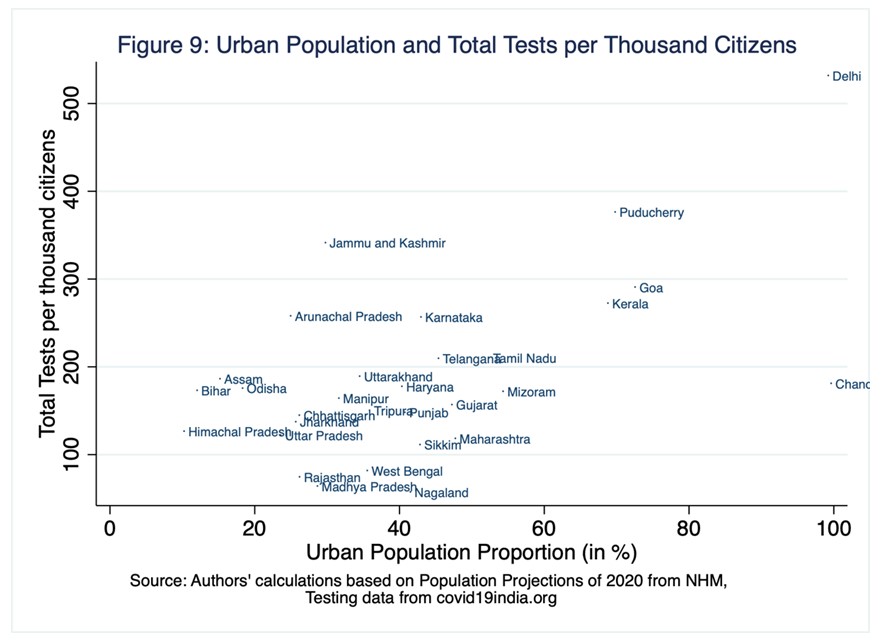
Once again, this is also observed in the scatter plot below. We find that the two variables don’t necessarily exhibit a strong relationship that can help us say that states with higher levels of urbanization saw higher levels of Covid-19 testing.
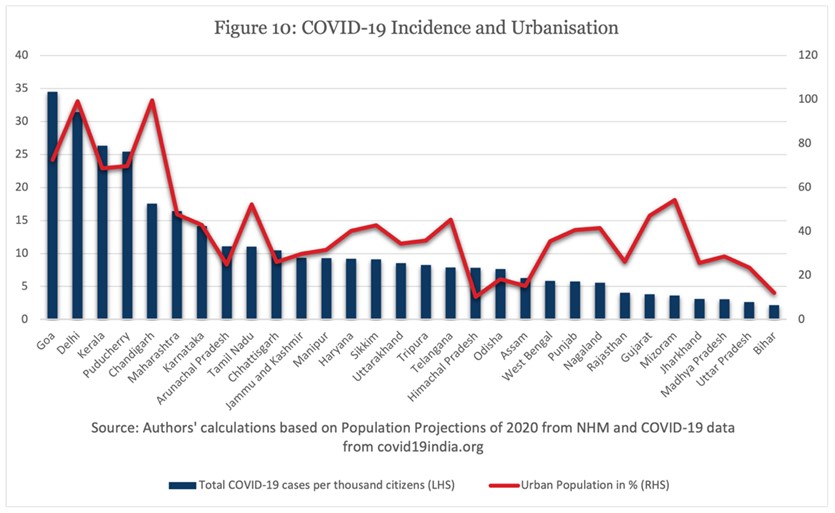
When we plot Covid-19 cases across states with urbanization on a graph however, we find that there is a higher linkage between the two variables. States with higher levels of urbanization have higher number Covid-19 cases per thousand population as seen in the chart below (Covid-19 Incidence and Urbanization)
Covid-19 testing in India vs the neighborhood
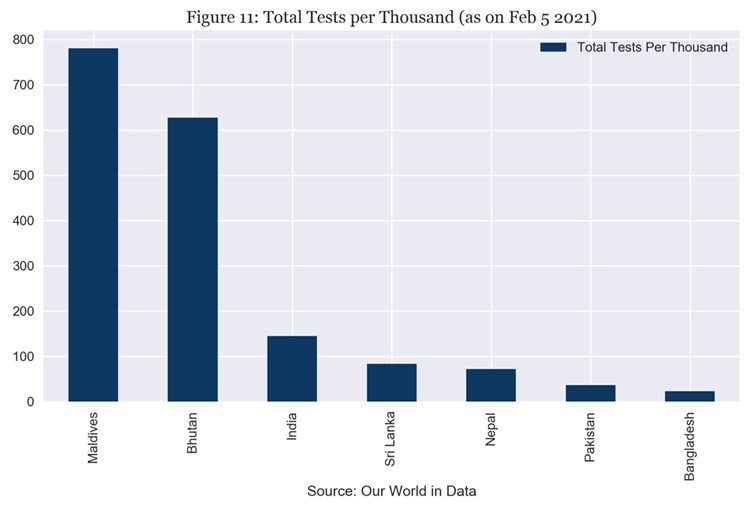
How does Covid-19 testing in India compare with the immediate neighborhood? Once again, we base our analysis on data sourced from Our World in Data.
According to this data, India has conducted 143 tests per thousand population till 1 Feb 2021. This number is 22 for Bangladesh, 81 for Sri Lanka, 71 for Nepal and 36 for Pakistan. Bhutan and Maldives have conducted 616 and 755 tests per thousand people.
Balakrishnan and Namboodhiry also studied the relationship between rankings of countries according to the death rate (Covid-19) and their rankings according to public health expenditure as percentage of their GDP. They found that“data from across South Asia also shows that there is a strong inverse relationship between the ranking of the countries according to the death rate and their ranking according to public health expenditure as percentage of GDP.”
Conclusion
After looking at data, we find that the decline in new cases can be attributed to lower levels of transmission and not to lower levels of testing.
We also find that the levels of testing across states is not influenced by the per capita NSDP of the state. Moreover, a similar lack of correlation is seen between the level of urbanization in a state and the total number of tests performed.
At the same time, we can see from the Balakrishnan, Namboodhiry article that there is a strong correlation between the states’ expenditure on public health and Covid-19 fatality. This correlation is also observed in India’s neighborhood.
India has entered February 2021 with the vaccination effort moving to frontline workers. According to Our World in Data, India had vaccinated 0.42 per cent of the population till 6 February 2021. Israel leads the world with 62.9 per cent of its population having received at least one jab of the vaccine.
For policymakers, a sharp decline in new cases and a ramping up of vaccination efforts can be helpful in deciding on relaxation of any lockdown measures. There are concerns, however. The two new strains of Coronavirus detected in the UK (B.1.1.7), and South Africa (501Y.V2) can complicate such decisions.
Existing vaccines have performed well against the UK variant, but the South African strain has not been met with much success so far. The Oxford/AstraZeneca vaccine (being administered in India as Covishield) has not been effective against the South African variant according to a study reported in the media. This has led experts like Dr Ashish Jha, Dean of Public Health, Brown University to warn about these mutations. The first step that Dr Jha suggests is ramping up vaccination.
For India, this means three things: scaling up vaccination, constant vigilance and an increase in public health expenditure. The government has allocated an additional Rs 64,180 crores over the next 6 years to improve primary, secondary and tertiary healthcare in the country. The budget also provides Rs 35,000 crore for Covid-19 vaccines.
To keep the number of new cases down, India will need to continue testing at current levels for Covid-19 while trying to vaccinate the elderly (aged above 50) and the more susceptible population (those with co-morbidities) at the earliest.
Endnotes
[i]Economic and Political Weekly, 6 February 2021
If you wish to republish this article or use an extract or chart, please read CEDA’s republishing guidelines.